

Typical Operative Report
As promised, I have included a typical operative cataract report in this post (it has been stripped of all identifying information). For anyone outside of the field of ophthalmology reading this will most likely be as clear as mud. Don’t worry, over the next few posts I will clarify this post in excruciating detail. When you are done reading this series of posts, you’ll probably know more about how cataract surgery is done than your own internist.
Procedure in Detail:
(Note: Blue italicized texts in brackets are not part of the report. They merely show the article series sections)
[Prior to cataract surgery]
Preoperatively, Nevanac, Vigamox, Omnipred 1% drops were prescribed or given to the patient to use in the left eye four times a day beginning four days prior to surgery. On the morning of surgery, the following drops were placed in the patient’s left eye every 10-15 minutes x4 beginning approximately one hour prior to surgery: Mydriacyl 1%, Phenylephrine 2.5%, Vigamox, Nevanac.
[Getting ready for the actual cataract surgery]
The patient was transported to the operating room in a supine position on a Stryker gurney. Once in the operating room, Tetracaine 0.5% drops were placed in the left eye following which Xylocaine 2% jelly was placed in the fornices on the left. The microscope was moved into position and the patient was asked to look at the microscope light which she was able to do without difficulty. The microscope was moved out of position and the patient was prepped and draped in the standard sterile fashion using a povidone-iodine solution over the left face and lashes and a Betadine 5% ophthalmic solution in the fornices followed by a sterile saline rinse. Steri-Strips were used to drape the lashes out of the operative field, following which Tegaderm was placed over the left face through which a lid speculum was placed.
[Start of surgery]
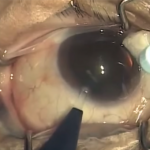
The microscope was moved back into position and a paracentesis was created at the one and five o’clock positions through which 0.3 cc of Epi-Shugarcaine was injected into the anterior chamber. Viscoat was then injected into the anterior chamber firming up the globe. A clear cornea temporal incision was then created with a metal keratome following which a continuous curvilinear capsulorrhexis was created using a bent needle cystatome on a Provisc syringe followed by capsulorrhexis forceps.
[Actual cataract removal]
Hydrodissection and hydrodelineation were then completed with a visible fluid wave and good nuclear mobility noted. Phacoemulsification of the nucleus was then completed using a horizontal chop phacoemulsification technique requiring 0.7 minutes of phacoemulsification at 19% power. The remaining cortex was then removed using bimanual automated irrigation and aspiration.
[Placing the new lens into the eye]
Provisc was then injected into the anterior chamber and capsular bag following which the lens was inspected for proper power and good integrity. The lens was placed in the insertion device which was used to insert the lens through the temporal incision, guiding the leading haptic into the capsular bag. The trailing haptic was positioned in the capsular bag using a lens manipulator. The remaining viscoelastic was then removed using automated irrigation and aspiration, taking care that no residual viscoelastic was trapped behind the optic.
[Placing the suture]
A single 10-0 Vicryl suture was then placed in the temporal corneal incision and the knot was buried in the corneal stroma.
[‘close’ and double-check]
The incisions were then hydrated and the anterior chamber was formed to physiologic pressure (confirmed by intraoperative tonometry) at which pressure the incisions were checked and felt to be watertight and of good integrity. The lid speculum and drapes were then removed followed by placement of Vigamox drops in the fornices on the left. A shield was then placed over the left eye which the patient was instructed to keep on the eye except during placement of Nevanac, Vigamox, Omnipred 1% drops which she is to use including the day of surgery. She was instructed to avoid any heavy exertion and is to follow up in my office the day after surgery. She tolerated the procedure well.
© 2009 David Richardson, MD





Leave a Reply