

Actual Cataract Removal
Finally, it is time to remove the cataract:
Hydrodissection and hydrodelineation were then completed with a visible fluid wave and good nuclear mobility noted.
‘Hydrodissection’ is a technique used to free the cataract from its attachments to the capsular bag. Without freeing the lens, all surgical forces that act on the lens would be translated through the capsule to the zonules (the delicate cables that hold the lens in place). If these zonules are damaged during surgery then there will not be sufficient support to place a clear new lens in the eye.
During hydrodissection fluid is injected between the capsule and lens. This fluid travels around the lens creating a space between it and the capsule. If this step is not completed the remaining steps of catarct removal are more difficult and dangerous to perform.
Hydrodelineation is very similar to hydrodissetion except the layers separated are those of the lens nucleus (hard, central part of the cataract) and epi-nucleus (softer outer part of the cataract). This step does not have to be performed unless the surgeon uses an advanced technique call ‘phaco-chop’ (more on that next).
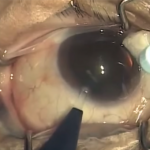
Phacoemulsification of the nucleus was then completed using a horizontal chop phacoemulsification technique requiring 0.6 minutes of phacoemulsification at 24% power.
Phacoemulsification is the ultrasound technology currently used by the majority of US surgeons. Essentially, a hollow tip vibrates at an extremely high frequency (faster than the speed of sound) breaking up the cataract into small pieces. These fragments are then vacuumed through the central opening of the tip and out of the eye. Other methods of breaking up the cataract do exist including laser and pulses of water. However, neither of these has really caught on in the US as the ultrasound works so well for most types of cataracts.
There is, however, a downside to ultrasound. If the tip of the ultrasound handpiece touches the capsule, the bag will tear allowing vitreous (the gel behind the capsular bag) to come forward. This is the main thing all cataract surgeons try to avoid as it often significantly complicates the surgery. Additionally, as discussed earlier, the ultrasound energy is not only absorbed by the cataract, but also by the cornea resulting in swelling. An advanced technique such as phaco-chop can reduce the total amount of ultrasound time used (compared to older and more basic techniques such as ‘divide and conquer’) and thus limit the amount of corneal edema.
The remaining cortex was then removed using bimanual automated irrigation and aspiration.
The cortex is that part of the cataract still adherent to the capsular bag. It has a stringy, tenacious character to it and is usually still present even with hydro-dissection. It must be removed or the bag will not be optically clear resulting in blurred vision and inflammation. However, the capsule is very delicate an tears with any significant traction on it. To get an idea of what this is like lay out some cheap plastic wrap (the stuff you use to cover leftovers before you put them in the refrigerator) and stick some painter’s tape on it. Now try to remove the tape without stretching or tearing the plastic wrap.
As you can imagine, this is another step in cataract surgery which has a high risk of ‘capsular rupture,’ resulting in ‘vitreous loss,’ or tearing of the capsule allowing the vitreous gel to come forward.
In order to decrease this risk I use a technique called ‘bi-manual’ irrigation and aspiration. This requires the simultaneous use of two instruments (rather than one) allowing me to obtain better control in the eye. Not every surgeon, however, uses the bi-manual technique as it requires (1) expensive handpieces that many surgery centers will not pay for (I own my bi-manual handpieces); (2) phacoemulsification equipment with excellent fluidics (a topic that would require its own post); (3) is technically more challenging to perform; (4) takes longer to complete than with ‘co-axial’ or one-handed irrigation and aspiration.
© 2009 David Richardson, MD





Leave a Reply