
Resource Speaker: Dr. David Richardson
When: Friday, January 8, 2016 from 11:00 AM to 12:00 PM
Where: Crowell Public Library – 1890 Huntington Drive, San Marino, CA 91108, United States
Dr. David Richardson talks about cataracts, cataract surgery, types of intraocular lenses, and laser cataract surgery or laser-assisted cataract surgery.
TRANSCRIPTION:
Very good. So, we’ll go head and start the program. I want to thank everyone for coming here today. On this beautiful day without rain. hidden inside. Room that has the shades down’s not exactly the ideal place to be but I’m hoping to make it worth your time.
So what we’re going to be talking about today is the topic of the book that I wrote that’s available here in the library for your borrowing. You can also get it online at Amazon. And for those who want to purchase it directly from us today, we’ll give it to you at our cost, which is $10 and any revenue that we get today will go to the library’s donation. So, basically if you wanted it, it’s available.
Now I’m going to give you information that, for the most part, is not in this book. This is information that’s relatively new but I will start with an introduction to what cataracts are and how cataract surgery is performed.
Before I do so, just to introduce myself and justify the reason why I’m giving the talk…
My name is David Richardson. I grew up in Southern California; went to USC for undergraduate and I’m an ophthalmologist, which means that I had to go to medical school before training to perform surgery on the eye. Presently, I’m an Assistant Professor of Clinical Ophthalmology at USC Keck School of Medicine. The adjunct just means that I’m also in private practice. My role there is primarily to train young surgeons on how to perform cataract surgery. I also have a private practice which is just down the street here at 2020 Huntington Drive.
Now, before we get to cataracts, it’s important to understand the eye itself. This is an image of the eye and just briefly the very front of the eye, which is the clear window of the eye, is the cornea. The cornea focuses light through the pupil, which is the opening and the colored part of the eye which is the iris through the lens. This here is the lens that sits behind the iris and it focuses light unto the retina which then sends the signal back through the optic nerve to the brain. Now, the lens in the eye is actually what becomes the cataract. So the lens, essentially, becomes less clear and as it loses its clarity, so do you.
So I find it’s helpful to think of the eyes is a bit like a camera for those who remember cameras. An object would essentially reflect light it would then be focused through the lens onto the film in the back of the camera and you can think of the eyes being quite similar.
So essentially the image is focused by the cornea – the front of the eye, through the lens which does additional work focusing the light on to the retina and then out through the optic nerve so what then really is a cataract?
What is Cataract?
Well, cataract is a term that actually means waterfall and back in the day, not so long ago, just a few decades ago, your cataract would actually have to get bad enough that anyone could see it and it would look at bit like a waterfall through the pupil. The natural pupil with a clear lens should be dark but with a significant cataract here, it actually reflects light back and looks a bit like water that’s being churned up. Looking again at the anatomical image in the eye you can see that the normal lens should be clear and focus light very well . Whereas as the lens in the eye (again it’s the actual lens) becomes more opaque it’s not able to focus light as well.
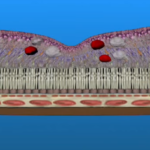
Here are some images of actual lenses as they become more cataractous with time. And this is pretty severe. We generally don’t let them get to this point anymore (this step) beyond that is actually the white cataract you saw the other image.
What are the symptoms of cataracts?
Well there are many symptoms and they range from just blurred vision, to cloudy or hazy vision. You can also have double vision or ghosting and glare or sensitivity to light especially with oncoming headlights or traffic lights at night. And then another common thing that tends to be an earlier occurrence, so it’s a bit more subtle, is yellowing vision. So blues become more green. Whites become more yellow.
When to consider cataract surgery?
If we don’t allow cataracts to get to that kind of brown or white tint stage, when should somebody consider cataract surgery? Well, in general we recommend that you consider it when what you call your activities of daily living are being impacted by the cataract. Now fortunate thing is that I don’t define activities of daily living. You get to define that. So what are the things that you need to do, want to do, enjoy doing that you’re no longer able to do even with a new pair of spectacles – that could be reading driving computer work but it could even be hobbies. You know if you’re a golfer and you don’t have to be a scratch golfer. If you enjoy it but you can no longer see your ball and it’s not because you’re looking at it but just because you can’t see where it’s going then it’s time to consider cataract surgery.
How is Cataract Surgery done?
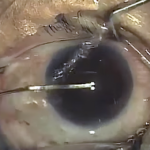
So then let me show you and animation of how cataract surgery is actually done. So essentially a small incision is made in the cornea and then the bag that holds the lens with the cataract is opened up (that’s called creating a capsulorhexis) An ultrasound device, which is very, very small little tubes that’s used to emulsify the cataract itself and then a new lens is placed through that small incision and allowed to unfold in the eye. So the surgery itself, on average, can take less than 20 minutes.
Now you’re generally in the surgery center for longer than that because it’s done under sterile conditions. You’ll probably have a little IV or something that will get you…just say that you’re relaxed you don’t care about what’s going on.
Types of Intraocular Lenses
Now you saw in that video that the lens was placed in the eye so it’s not just that your cataract or natural lens is removed it actually has to be replaced because if we didn’t replace it with a new lens you really still wouldn’t see well. You’d need coke bottle glasses.
Back in the day, about forty years ago, cataracts were just removed and everyone had these – what were called, “aphakic spectacles”, which looks kind of like Mr. McHugh spectacles. You don’t need that anymore. And as a matter of fact, it’s now possible with cataract surgery to actually achieve a level of vision without spectacles or contact lens correction. We’ll talk about that in a second.
So the actual lenses that are used – these are synthetic lenses so they’re not donated from other humans they’re not from animals. The common materials that are used here in the US are acrylic, silicon and collamer. The reason these materials are used is because they’re clear, they’re bio-compatible so the body doesn’t reject them and they’re flexible. The flexibility is important because the incision that’s used ** created in time of cataract surgery tends to be on the order of two to three millimeters. Very, very small incision.
In addition to different materials being used there are actual different types or functions of intraocular lens – also known as IOLs.
Different types or functions of intraocular lens
So let’s talk about some of these different functions. Roughly you can divide them into four groups Monofocal intraocular lenses, then toic and multifocal and what’s called pseudo-accommodative.
Monofocal Lens
Now the monofocal lenses have been around since Sir Harold Ridley in the UK first discovered the Royal Air Force pilots who had pieces of the windshield stock in their eye – clear pieces of this windshield, show their eyes were not rejecting these pieces of windshield. Amazingly the canopies just sat in the eye without inflammation. So Sir Herald Ridley, who was not a sir at that time, thought, “well this is this is really interesting. I wonder whether we could make lenses, actually, put in in the eyes of people who had cataracts.” And he did that and just about lost his license because at that time, putting anything in the body let alone in the eye was considered to be just absolutely hearsay. Fortunately for all of us his foresight turned out to be accepted by even the stodgy academic institutions and we now are all benefiting from that – that wonderful work of Sir Harold Ridley.
So these monofocal lenses replace the natural lens, they’re clear and they do focus light pretty well but they don’t focus it quite as well as you might need for all of your activities and we’ll get into why that is the main reason is that they don’t correct astigmatism and there are other aberrations in the cornea that can affect vision and that’s where spectacles and contact lenses can be of benefit. Now these lenses are covered by Medicare and all insurances but after cataract surgery with monofocal lens, unless your cornea has no astigmatism and is otherwise in perfect condition, you will likely need spectacles for most if not all of your activities. So again, these are well made high quality lenses. They just don’t do anything to limit your need for spectacles. So the next set of lenses I’m going to talk about is the set of toric intraocular lenses.
Toric Lens
Toric lenses correct astigmatism. Astigmatism is you can think of it as an irregularity of the cornea the front and the window of the eye the first surfaced that reflect -that refracts light so bends light rays to focus on the back of the eye and whereas a normal cornea is round kind of like a softball, astigmatic corneas are shaped a bit more like a football. Not enough that you could tell just by looking but if we measure, using very well (I’d say, we can measure using) very sophisticated equipment now. But it could be measured decades ago with with less sophisticated equipment you can tell that there’s some distortion there. Well what toric lenses do is they essentially balance out that cornial distortion so with a toric lens for those who have astigmatism end up with excellent, crisp vision at a particular distance.
So if you wanted to see well at distance, so far away, after cataract surgery and you had a astigmatism, a toric lens would allow you to have excellent vision at distance without spectacles or contacts. Now, it doesn’t give you a range of vision however so you wouldn’t be able to see necessarily at near but you could choose to set your focus it near and then you’d need spectacles for distance so the benefits of the toric lens provides excellent quality vision at a particular distance.
Limitations: It doesn’t provide a range of vision so you may still need cheaters if you choose to have it set for distance and it’s considered either a premium or refractive lens by Medicare and most insurances so the cost of the lens as well as all of the testing and surgical maneuvers and other things that are required to place or position the lens are not covered by Medicare and most insurance.
Multifocal Lens
Then there’s multifocal lenses. Now multifocal lenses, here in the united states have these little concentric rings you can probably see here now what these rings do is they actually focus distance images and near images on the retina at the same time. Now I don’t know who first thought of this because it’s a bit on intuitive to think that you could have two images focused on the retina at the same time and the brain would be able to choose which image is the image you should be looking at but amazingly most people who have these lenses implanted in their eyes do quite well and end up with a nice range of daytime vision.
The downside however is that not everyone adapts to the lens. The process is called neuro adaptation where as some cynical ophthalmologist had said neuro resignation because you do have these two images and you will always have either a small ghosts or a halo around the main image that you’re focusing on now that’s not usually an issue during the day but at night it’s particularly with driving people do notice little halos around lights.
Again, most people that have this, who have otherwise healthy eyes, really enjoy their range of vision but it’s important to know before choosing any particular lens what the strengths and weaknesses are. And again, this is not a lens that’s covered by Medicare or insurance. Then we have what are called the pseudo accommodating lens.
Pseudo-Accomodating Lens
Accommodation is the natural ability of your lens before you turn forty or fifty to be able to change focus from far away up to very close and actually as infants and toddlers we can focus very very close up with that ability to change the focus reflects the lens in the eye decreases with time until slowly it feels like our arms aren’t quite long enough and that’s what we need to start using the cheaters. We lose that accommodative effect.
Well pseudo accommodating IOL or intraocular lenses are quite flexible and as such they they seem to have some – we don’t really know whether its just movement or just some wild distortion or what it might be but they do you have more of a range of vision than the other lenses than the standard monofocal lens and because it’s not a multifocal lens so it’s not focusing two images on the retina at the same time there are no halos to be expected.
Now, the main pseudo accommodating intraocular lenses that are available in the United States are the crystalens, the star nanoflex and the Softec HDO. Europe has a number of others that we don’t yet have. We’re hoping that the FDA will approve them sometime over the next decade or so. Now, what are the limitations of pseudo-accommodating lenses? Well they don’t get quite the range that some of the multifocals do.
Generally, the pseudo accommodating lenses will focus from distance to about arms-length. Sometimes, you can get up to about 16 or 18 inches but if you want to have a fuller range of vision with the pseudo accommodating lens, you really have to have both eyes done so that when the eye is set for distance and it blends to intermediate the other eye, you can set a bit closer. So you get more of a near range. Between the two eyes you do end up with an outstanding range of uncorrected, that spectacle-free vision during the day. You may still need cheaters or readers for real small prints, conditions such as low light conditions. But in general for those who think that they might not be good candidates for the multifocal lens because they’re worried about the Halos at night or if you have other conditions in the eyes such as some mild macular degeneration, glaucoma, dry eye, blepharitis – none of those conditions play very well with the multifocal lens, you can still have a pseudo accommodating lens and achieve some spectacle independence. And again the procedure itself for implanting and testing and all of that for pseudo- accommodating intraocular lens is generally not covered by insurance or Medicare. Now it’s worth noting, since I’ve been talking about the limitations because I consider it very important with my patients that they understand what the limitations are. I do not want the surgery to go perfectly well and have someone disappointed because he or she was expecting that the current technology was capable of providing more than it is.
There is currently no lens available on the market either here or in Europe or you know some other country that doesn’t have this strict regulation that can provide the full range of uncorrected vision, in all lighting conditions without the need for spectacular contacts and that’s true of the lenses that we put in the eyes. it’s true of the cameras that we have – the camera phone or 4d high-definition you know cinema quality video camera. The way our eyes are able to adjust almost instantaneously when we’re young, younger than say you know thirty or forty to any light condition and almost any distances is absolutely phenomenal and we just don’t have the technology , material technology or digital technology to to recreate that. But we’ve we’ve managed when it comes to intraocular lenses to provide a pretty good functional range in the right lighting conditions. But you have to understand that we as humans expect a lot of our eyes and so what can you expect?
If you decide to go with one of those lenses that I just spoke about whether it’s a multifocal, Toric or pseudo-accommodating lens, you will still need to have spectacles for what we consider to be the extremes of vision. Extremes of vision meaning very low light or conditions where you’ve got low light and then suddenly there’s bright light. Think about nigh-time driving for instance.. And then certain extremes of reading so if you’re gonna try to read something… like if you’re a cartographer there’s no lens that we have available to provide that kind of ability to see tiny little subtle markings on a map four inches from your eyes but for most of our activities when it comes to reading iPads or your iPhone or computer or your dashboard driving during the day, we can provide a nice range available for those activities.
So those are the lenses that are available today, here in the US. Kind of general categorization of them but of late, there’s been something else that’s created quite a bit of buzz among those who are considering cataract surgery and that is laser cataract surgery. So if you’ve heard anything about laser cataract surgery you’ve probably heard some pretty amazing things about it that it’s more precise, its gentler, it’s safer – just all of these these terms that make you feel that this is just, you know, so much better than cataract surgery has been for decades and you know it should be because I have laser cataract surgery means that in addition to the cost of cataract surgery which may be covered by insurance in addition to the cost of the premium lens package if you choose that you’re going to have to pay for the use of a laser, which could be as much as $1,500 and in general surgeons are charging somewhere between 800 and $1,500 per eye to use the laser. Now here’s the interesting thing you might not even have the option to pay for the laser it turns out that medicare does not allow the surgeon or the surgery center to charge extra for using the laser if you’re going with the standard lens and don’t have some kind of refractive issues such as astigmatism. You may think this is not fair there’s a lot of things that that medicare does that’s unfair but medicare actually restricts the ability to have it so is that an issue should you be upset if you are thinking that you’re just gonna go with the monofocal lens but you want the laser? Is that something that you should feel that you’re getting second-rate treatment for? Well, let’s take a look.
What is Laser Cataract Surgery
First of all, in order to answer that question we have to look at, “What is this laser cataract surgery?
Well laser cataract surgery is really a misnomer because those surgery is not done by a laser. Its laser assisted cataract surgery. The laser performs certain parts of the surgery but you still have to use ultrasound which is called phacoemulsification in order to take the lens out. So why then is there all of this haballo about laser cataract surgery or laser assisted cataract surgery – also known as FLACS which stands for femtosecond laser assisted cataract surgery because it’s a particular type of laser called the femtosecond laser and a particularly expensive type of laser.
There are currently four companies that make femtosecond lasers that are available here in the US. Each one of these lasers has a price tag of approximately a half a million dollars. On top of that the laser company charges either the surgeon or this surgery center between $300 and $900 per use. So every time it’s used on an eye, they charge what’s called a click fee. Well you can imagine that if you’ve got this device sitting around using up a room you not gonna want it to be a half a million dollar paperweight. So so you’re going to tell people that this is the absolute best thing around since sliced bread and the question is, is it?It could be. Let’s take a look.
What does the laser do?
So what does the laser do in order to figure out whether or not it’s worth this we have to look at what it does. Well it creates corneal incision so that that two to three millimeter incision the cornea that you have to make in order to get to the lens will traditionally we make with what’s called a keartone – a handheld instrument it’s made of either metal or gym quality blades – sapphire, diamond things like that and these blades are disposable and they’re very sharp. If they’re metal you use it at once. You toss it. If it’s a diamond, it’s sharp and like diamonds, it stays sharp. And it makes a wonderfully, wonderfully just precise incision that seals on its own. So it’s a great incision and the laser does the same thing and it’s really cool to watch it make the incision.
Does it make a better incision? Unfortunately there’s no objective evidence that the incision is a better incision. What else does it do? Now this is actually interesting the incision is is is kind of an extra but in order to get to the cataract, you have to make an opening in the capsular bag. The capsular bag is a very very delicate transparent membrane and it’s very very thin it’s on the order of microns, right, thousands of a millimeter. It’s incredibly delicate and this is the part of surgery that gives most cataract surgeons early in their career coronaries. So to residents that I trained this is the most difficult part of the surgery and if it’s not done well the whole rest of the surgery is impacted. I can tell you that isn’t attending when I’m watching the residents I can feel my coronary state. But once you’ve done a few hundred cataracts, this should not be an issue anymore and most capable surgeons are not fearful of making a round capsulorhexis.
So, what’s new about the laser? Well it makes a perfectly round capsulorhexis. I mean it’s perfectly round and so in terms of precision it’s beautiful to watch does it matter whether capsulorhexis is perfectly round? Well, when these lasers first came out there was a lot of of talk about it it should but it turns out it doesn’t. So it’s really pretty but it doesn’t make any difference in terms of final visual outcome. Now if I knew that my surgeon was uncomfortable making a capsulorhexis, then I might choose to have the laser instead of the surgeon make the capsulorhexis manually. Just like you know if you got somebody is not very good driving a stick best to have them drive the automatic but would rather just find somebody who knows how to drive the stick?
So we’ll talk about that. It can offer also soften the cataract. This is important because we know that the more energy that’s absorbed by the cornea, the more inflammation there is in the eye, and the longer it takes the eye to heal. Now the older techniques of ultrasound, called phacoemulsification – the other techniques such as divide and conquer where you make a couple of grooves then you split up the cataract took a lot of energy. The newer techniques, which are a bit more advanced and have a steep learning curve such as a chop, use a fraction of the energy of divide and conquer. So for the surgeons who still use divide and conquer, breaking up the cataract with a laser makes a lot of sense. Because they don’t have to use as much **** but for those surgeons who use the more advanced techniques you’re really not saving much energy in terms of ultrasound and recent evidence suggests that the eye doesn’t care what form of energy is used whether it’s ultrasound or whether it’s Electromatic magnetic laser energy it’s still energy and the eye responds to both the same. So it’s kind of like are you gonna pay for something in dollars or Euros.Well if it’s the same price does it really matter and it doesn’t seem to matter to the eye.
Now, there is one other thing that that the laser does. I mentioned earlier that it makes incisions in the cornea. Well it can make what are called Arcuate incisions that can correct astigmatism and this is how many surgeons are getting around the medicare issue of not using this laser and charging for it if you’re using a monofocal lens. Well, you have a little bit of astigmatism, let’s correct that. Well it turns out you can correct astigmatism with a diamond knife or a metal knife in the office or any operating room or you can use something you’ve all heard of before PRK photorefractive keratectomy or LASIK.
So ultimately what does the laser do? And the answer is nothing that couldn’t already be done without the laser. But you say what about this more precise, is safer, is gentler? All marketing terms with little evidence based on facts.
Now precise just means that as I said that capsulorrhexis is perfectly round. Yes, the laser can make a capsulorrhexis that is more round. You know, if you could get tiny little compass in the eye and drive the laser would do a better job than I can by hand just like any one of us is not an artist he tries to draw a circle is not going to draw as perfect circle as you would using a compass on paper. But it doesn’t matter or at least we don’t have any evidence to suggest that it matters. Gentler? What does that mean?That’s a term that has no meaning in surgery and one could argue actually it’s not as as gentle because in order to use the laser you have to dock it onto the eye and that provides quite a bit of pressure and when the dock comes off, most people have eyes look kind of bloody. It doesn’t look gentler to me. How about safer? Oh, this is a term that we can actually address. Because something that’s safer should have fewer complications. Right?
So, it turns out that FLACs may actually be less safe than cataract surgery performed with only an ultrasound. So, the Europeans – The European Society of Cataract and Refractive Surgery actually ran a study called the FLACS ESCRS study and what they found after performing this study in 16 centers, 10 European countries and almost 3,000 laser cataract surgery so it wasn’t a small little study. This was a big study, they found that when compared to ultrasound only cataract surgery (the kind of cataract surgery that’s been done for decades without a laser) those who had laser-assisted cataract surgery actually had worse vision after surgery compared to those who had ultrasound only.
But in terms of this safety issue it was quite clear that those who had a laser assisted cataract surgery had more postoperative complications. So by definition it’s less safe and here’s the interesting thing the whole point of having cataract surgery is to improve your vision but it turns out it with any surgery. Whether you’re exchanging a joint or a lens, not all surgeries work and occasionally people will end up worse off than before surgery. That’s something you absolutely want to avoid or minimize. Well it turns out that those who had laser assisted cataract surgery were actually more likely to have vision after surgery that was worse than the vision they had before surgery. Again this is a very very small number but doesn’t have to be a very large for it to be something that you want to avoid.
What Do I Recommend?
So what do you do when it comes to time to think about cataract surgery?
What do I recommend first of all I recommend that you find a skilled cataract surgeon. How do you find a skilled cataract surgeon? Well if you look at page 69 in the back of my book which again is available here at the library tomorrow I’ve actually created a section on how to choose a cataract surgeon. If you don’t want to borrow the book or buy it then I believe that I have that information available on my website online too. So that’s the most important thing – It’s finding a skilled cataract surgeon.
Two, choose an intraocular lens that meets your needs. All surgeons including myself have their preferences in terms of what lens they’re most comfortable with. But you now have the basic information necessary and you can find more online through more research as to which lens would best meet your needs and only you know what your needs are. For example, somebody who doesn’t drive at night much you know multifocal lens could be a very good option for you but if you’re in airline pilot that’s probably not going to be a great choice.
And then don’t fret about the tools that your cataract surgeon uses When you take your car in to get it fixed, you find a good mechanic. Do you care what particular brand of tool that mechanic is using so long as your car is reliable and working well afterwards No. And so the same thing should be true of your cataract surgeon and this also goes for other surgeons also and then most importantly, is after you’ve had that surgery, enjoy the vibrant, crisp beauty of the world around you because that’s ultimately what you’re doing this for.
Thank you




Leave a Reply